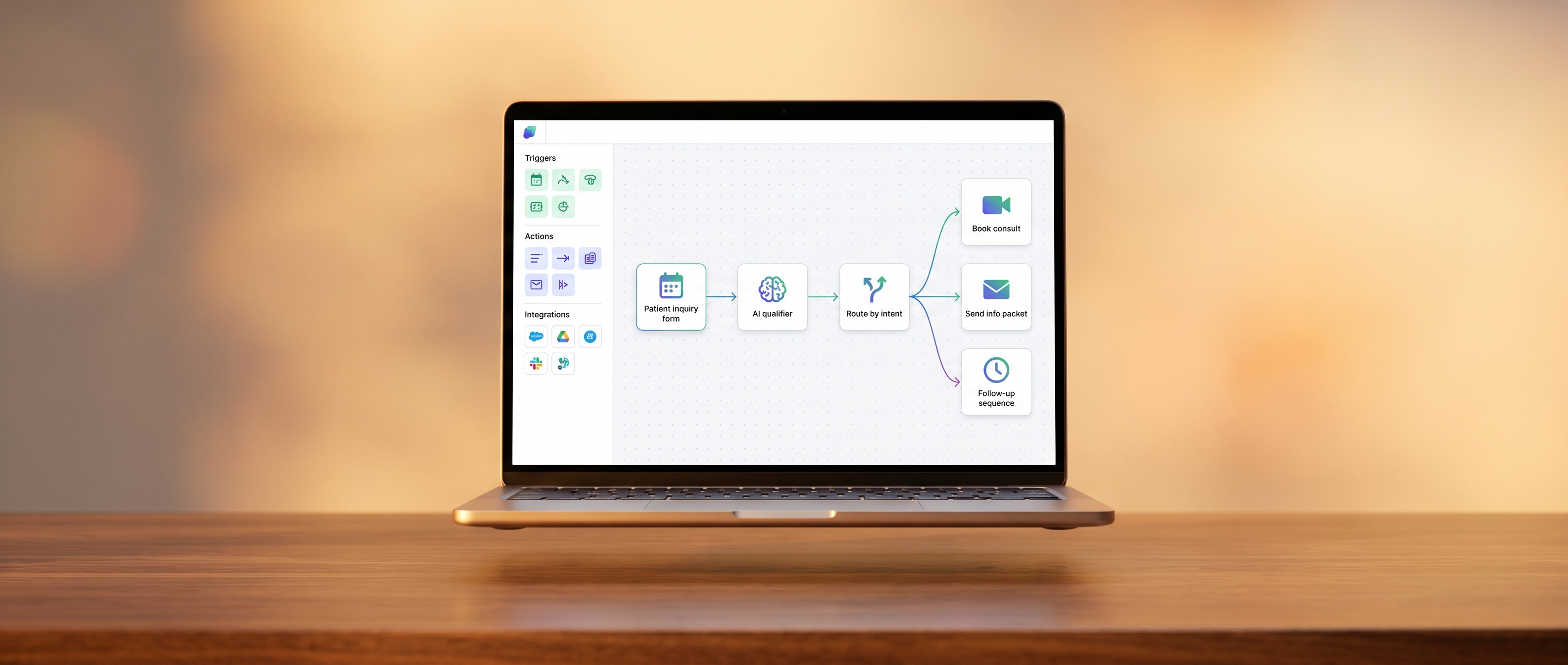
01The overview · How it works
The most expensive employees you'll never have to hire
AI agents got reliable enough in 2026 to handle real workflows, not chatbot toys, real workflows. Connect a CRM to a review system to email to call tracking. Triage incoming inquiries 24 hours a day. Recover quotes that didn't book. Generate reports that used to take a marketing person three days every month. The practices that build this infrastructure now will operate at a different scale within a year. The ones who don't will keep paying people to do work that should have been automated.